Hello again everybody.
Well, we hope you all have been learning over the course of our discussion. This next topic we are going to discuss is the crux of our investigation. We are comparing the use of NMES (post surgery) on quadriceps strength combined with a voluntary exercise program. The evidence supporting this discussion was viewed around subjects who either had Anterior Cruciate Ligament reconstruction (ACLR) or Total Knee Arthroplasty (TKA).
So let’s dive right into the information.
Although specialists continue to make efforts towards improving current rehabilitation techniques and developing new interventions to maximize quadriceps output following ACLR/TKA, a universally effective approach by which to restore pre-injury muscle strength has not been revealed (Palmieri-Smith, Thomas et al. 2008). So where does that leave us?
Well, we have established there is no exact method of rehabilitation, however, there are a variety of techniques that have established significant results, and additionally, there is marketable evidence that supports the use of NMES in combination with voluntary exercise.
The primary objective of a post ACLR or TKA is to provide a rehabilitation program that restores knee function to its optimum level. These objectives/goals are a challenge, as many patients return to sport or Activities of Daily Living (ADL’s) with persistent neuromuscular deficits, which ultimately include:
· Quadriceps weakness (being the most common)
6 months post ACL surgery, quadriceps strength can diminish by 20%, which is a major deficit for an athlete returning to a competitive level of sport (Palmieri-Smith, Thomas et al. 2008).
So why does this happen? According to Palmieri-Smith and colleagues (2008) there are two underlying reasons, which include:
 |
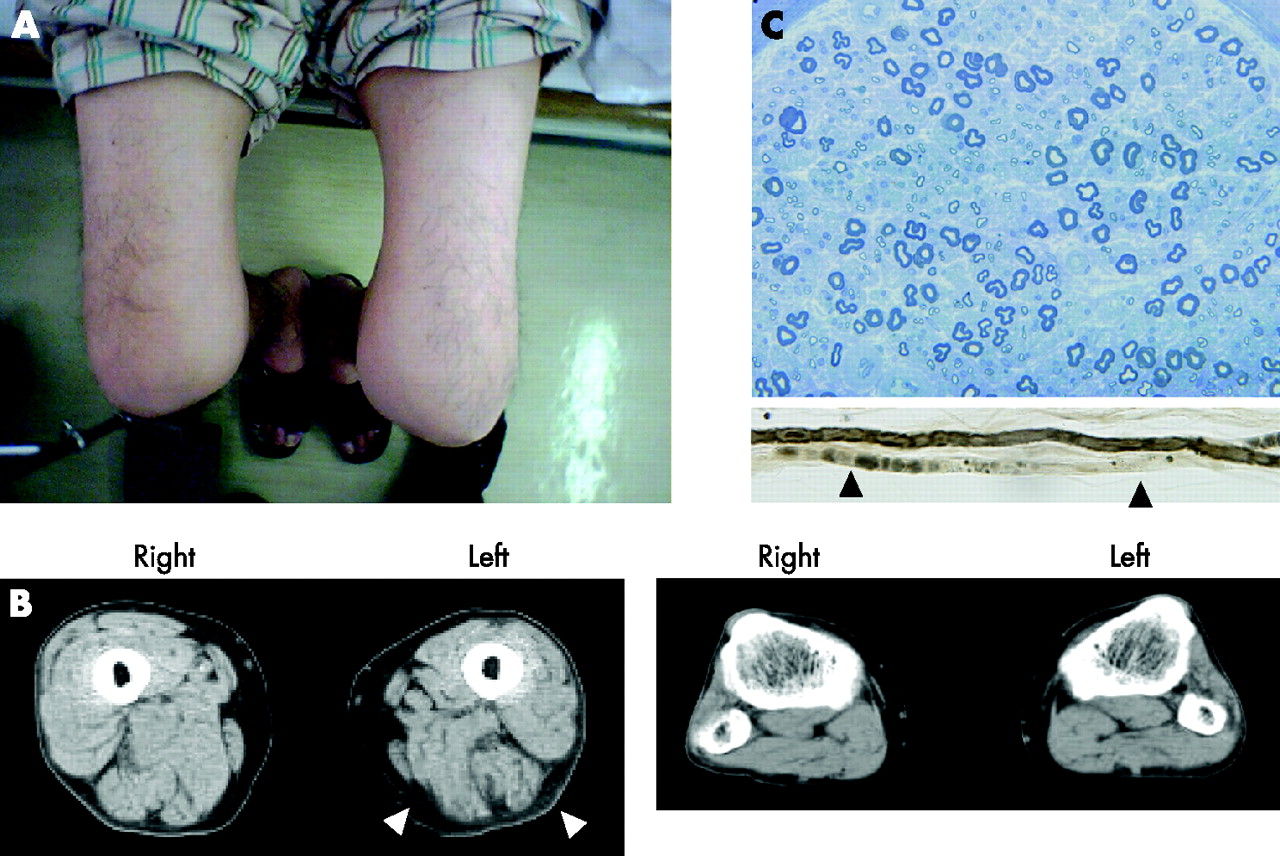
Figure 1: Demonstrates muscle
atrophy in the (R) quadriceps |
· Muscle atrophy, which is due to lack of use.
· Arthrogenic Muscle Inhibition (AMI), which simply refers to voluntary muscle activation failure
o Specifically, the decrease in mechanoreceptors from the ACL affects the reflex activity between the ligament and the quadriceps, resulting in an inability to actively recruit high-threshold motor units during voluntary quadriceps contraction.
With the use of NMES, the goal for rehabilitation is to target AMI. How is this done?
· NMES directly activates the motor axon and recruits the inhibited motor neurons
· Additionally, a greater number of Type 2 muscle fibres are generated which produce a greater force production in the quadriceps muscle
So what does the literature reveal about ACLR and TKA and the use of NMES as an adjunct treatment for rehabilitation?
A study by Synder-Mackler and colleagues (1995) established that four weeks of high intensity electrical stimulation combined with active exercises resulted in the following;
· 70.1% quadriceps strength at 2 months post reconstruction
· Subjects who performed only voluntary exercises only demonstrated 46.7% quadriceps strength
In addition Delitto et al (1988) reported the following findings at 8 weeks post ACL surgery:
- Subjects receiving NMES therapy had an isometric quadriceps strength of 78.8%
- The active exercise group only produced an isometric strength of 51.7%
Additional findings to Synder-Mackler and collegues (1995) revealed an Improvement in functional outcomes, including:
- Patients who had received NMES walked with a faster cadence and velocity
- A more functional knee flexion excursion
Therefore, it is clear that existing literature supports that NMES combined with active exercise is more effectual than active exercise alone in the restoration of quadriceps muscle (Palmieri-Smith et al, 2008).
There are some pit falls to the use of NMES in these studies. According to Fitzgerald et al (2003) one of the major concerns is that patient’s struggle to tolerate the protocol. The underlying reason for this is that some patients had undergone patellar tendon auto-graft ACLR, which specifically effected the position the knee is placed in during treatment (flexed between 60 and 90 degrees), whilst being connected to a dynamometer (measures force/power). As a result, Fitzgerald and colleagues (2003) produced a modified NMES protocol. The general protocol used can be seen in our first blog. The protocol used by Fitzgerald and colleagues (2003) involved placing the knee in extension, not connecting the patient to a dynamometer (reduces set-up time), as well as modifying the stimulus amplitude. The amplitude was increased till a full tetanic contraction of the quadriceps was evident, with an additional superior patella glide. At this point the amplitude was increased to the patient’s maximal tolerance level. All other parameters were consistent with traditional methods as seen in blog 1.
So, what results were produced with this modified protocol?
- NMES patients revealed a higher quadriceps index compared to the exercise group
- NMES group demonstrated higher ADL’s at both 12 and 16 weeks post surgery
- NMES subjects (at 16 weeks) achieved the clinical criteria to advance to agility training exercises compared to the active exercise group (Fitzgerald, Piva et al. 2003).
Evidently, this literature reveals that there can be slight complications with the application of NMES, however, as Fitzgerald and colleagues (2003) demonstrate there are ways of modifying (advocating for your patient s) the application of NMES whilst reaping the full benefits of the treatment.
Currently, the question researchers ask is; how long does the quadriceps strength gain last once NMES treatment has concluded? Simply, the research reveals that there is still considerable strength in the short-term (first 4 to 8 weeks), post ACLR treatment, but long –term still requires more investigation. However, a study by Steven et al, (2004) looked specifically at the benefits of NMES post TKA and established that quadriceps strength gains were still present at 6 months following treatment.
In summary, to maximize quadriceps strength, specialists need to incorporate methods to reduce muscle atrophy and AMI. If these factors can be reduced quickly following ACLR/TKA a more successful and efficient recovery will transpire for patients. Overall, we can see from the evidence provided that NMES therapy (traditional or modified protocol) combined with voluntary exercise, for post ACLR/TKA rehabilitation is a beneficial modality to increase quadriceps strength.
Stay tuned; next week, for our final post, we’ll be comparing the use of NMES in different aged populations (young and old) and the differences in benefits/affects between male and females.
Thanks for tuning into this week’s discussion, we hope you all enjoyed it and we’ll see you again next week.