|
Figure 1. NMES knee/quadriceps setup |
Jasraj Sidhu and Ben Takken
Hello everybody!!! As your hosts, we will be discussing the wonderful world of NMES over the next several weeks as it relates to quadriceps rehabilitation post knee surgery. We will be tackling this topic for a few different angles, and will be exploring some of the past and current literature that exists surrounding this modality as an effective therapeutic/rehabilitative tool. We thought that before taking you on this journey and getting into some deep discussion and debate, we would take this first opportunity to explain to you, the viewer, some of the basic uses and parameters involved with NMES. With this we hope to create a strong foundation on which we will continue to build and present further information. So without further ado, LETS GET STARTED!!!
What is NMES? How does it work?
NeuroMuscular Electrical Stimulation – creates an electrical impulse that stimulates specific muscles/muscle groups in patients who have difficulty with voluntary muscle contraction. It works by producing a mild electrical current that is carried through the skin to the muscle (Figure 2) leading to nerve depolarization and subsequent activation of muscle fibres (Bax, Staes et al. 2005).
 |
| Figure 2. Current transmission resulting in muscle activation |
Why is NMES useful?
 |
| Figure 3. Typical quadriceps NMES setup post knee surgery (Biphasic/Pulsed) |
In the case of quadriceps rehabilitation post knee surgery, NMESs’ purpose is mainly to prevent atrophy of the affected quadriceps muscles due to disuse during healing (Bax, Staes et al. 2005). This is a common occurrence with patients falling into one or more of the following categories; muscle non-use, post-surgery (Figure 3) and/or incomplete spinal injury. Additional beneficial claims surrounding its use include (Bax, Staes et al. 2005);
· Re-educate muscle (rhythm/timing) and neurological stimulation.
· Limit effect of joint pain/inflammation on muscle contraction.
· Recruit maximal muscle fibres during strengthening exercises (NMES alone or combined with exercise? We will be getting to this in some detail on!).
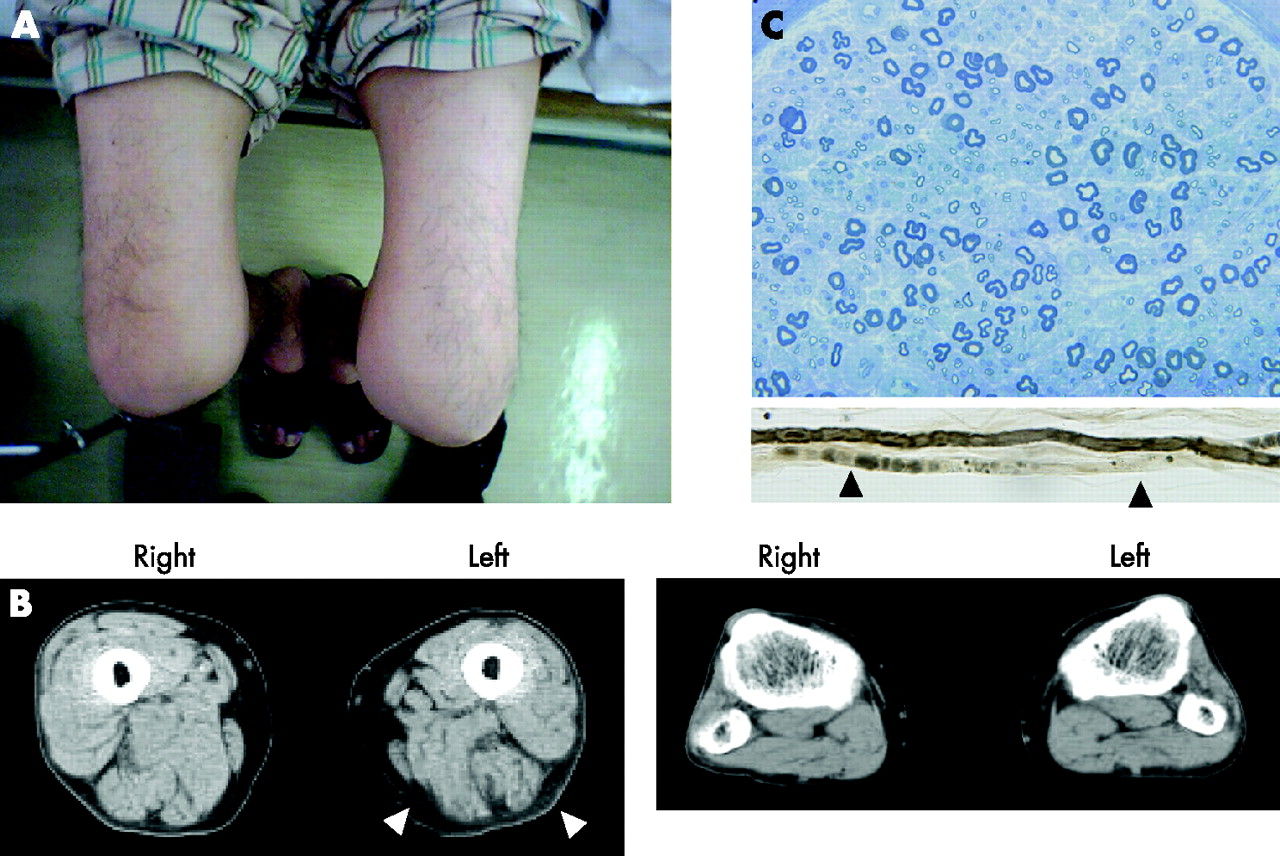
· Control oedema with NMES initiated muscle contractions; help to pump blood through the tissue (Figure 4).
 |
Figure 4. Odema as a result of postoperative knee surgery. The use of NMES can reduce extent of swelling via activation/stimlation of the muscle pump to aid in fluid clearing.
|
Do multiple parameters exist for NMES?
YES!!! The two common setups of NMES are; Russian and Biphasic/Pulsed, both of which have their own separate parameters and functions.
· Uses high frequency for deep muscle stimulation via activation of the motor nerve (Figure 2), thereby resulting in a more forceful muscle contraction.
· Implications for improving muscle strength predominantly in intermediate to late stages of post knee surgery rehab (Laughman, Youdas et al. 1983).
Typical Dosage
Carrier Frequency | 2500Hz |
Frequency | 75Hz |
On time | 10-15sec |
Off time | 50-120sec |
Ramp | 2sec up:2sec down |
Amplitude | As tolerated |
Number of contractions | 10-15 |
Sessions/week | 3 |
Biphasic/Pulsed;
· Used to maintain ROM, muscle re-education, preventing joint contractures or muscle atrophy, increasing blood flow, pain management and decreasing muscle spasm (Rebai, Barra et al. 2002).
· Greater implications for early to intermediate stages of post knee surgery rehab (Rebai, Barra et al. 2002).
Typical Dosage
Pulse Duration | 400-600 microseconds |
Frequency | 75Hz |
On time | 10-15sec |
Off time | 50-120sec |
Ramp | 2sec up:2sec down |
Amplitude | As tolerated |
Number of contractions | 10-15 |
Sessions/week | 3 |
Are there any contraindications/precautions to NMES?
According to the Australian Physiotherapy Association, the following contraindications/precautions should be followed when applying NMES (Robertson, Chipchase, et al. 2001).
Contraindications;
· musculotendinous lesion*
· absence of a secure bony attachment of the muscle*
· superficial metal*
· over upper thoracic region
· cardiac pacemaker
· over carotid sinus of neck
· uncontrolled hyper/hypotension
· DVT*
· Abdominal/lumbosacral/pelvic region during pregnancy
· Infection*
· Prone to seizure
· Transcranial stimulation
· Stimulation over eyes
Precautions;
· Reduced sharp/blunt discrimination*
· Broken skin*
· Repeated uses of self-adhesive electrode sponges and covers
*pay close attention to as a result of postoperative knee surgery (possible complications?)
OVERWHELMED YET!? Well don’t be, today’s post was simply to provide you with a little bit of background concerning the basics of NMES. Over the next few weeks well will be discussing topics specifically looking at quadriceps rehabilitation in post knee surgery patients as it relates to NMES use. These topics will explore;
· Does NMES improve quadriceps strength post knee surgery?
· NMES versus Volitional Exercise versus Combined program
· Application of NMES across different populations: implications of gender and age differences